The image below is of a horse's foot that is suffering from a conformational problem known as "long toe-under run heels". This horse tends to grow significant amount of hoof wall within 4-5 weeks without growing normal heel. Although the heel regions grow, they tend to roll under the center of the hoof. As such, this horse and others like him are prone to heel pain and poor performance. In Figure 1 the center of rotation is marked by the blue line. Ideally, the length of foot that is in front of the blue line and behind should be equal. This would result in a horse that is balanced "cranial to caudal" with respect to the center of rotation.
 |
| Figure 1 As the amount of foot behind (B) or caudal to the center of rotation decreases compared to "A" there is a significant increase in the amount of force that is applied across the heel regions. This results in the rolling under or "under run heels" that is imaged in Figure 1 and 2. When this horse is trimmed, the hoof wall needs to be trimmed back to the widest portion of the frog. This may seem counter intuitive due to the apparent "lack of heel" however it is necessary to achieve "normal" heel growth. |
 |
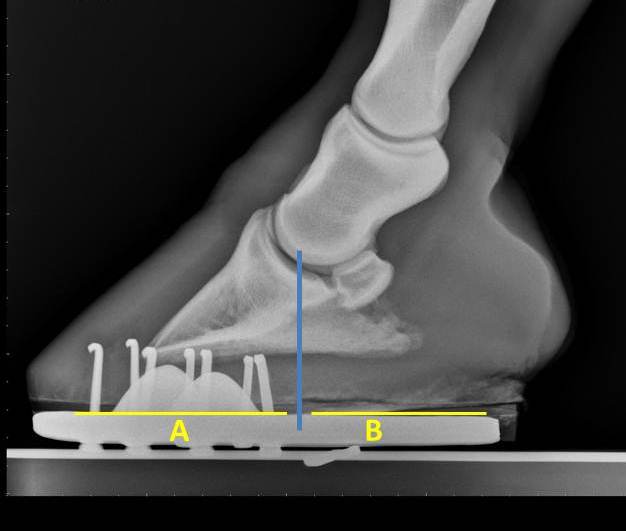
| Figure 2 The radiograph below is that of horse that has heel pain and is lame when trotted in a small circle in both directions. The hoof tester exam noted a strong positive response across the bar region of both heels. Notice that the length of "B" is significantly shorter than "A". In order to correct this problem, corrective shoeing is a must! The process begins with a balanced trim that includes lowering the heels to the widest portion of the frog. This is followed by applying a shoe that either has built-in break over such as a natural balance/equilibrium shoe or break over is increased manually be rolling the toe. In addition the shoe is set extra full in an attempt to increase the length of "B" and hence support the caudal aspect of the foot. |
 |
| Figure 3 In Figure 4 the horse has been trimmed and re-set. Notice that the length of "B" is nearly the same as "A". This horse is quite close to being balanced with regard to the center of rotation (blue line) and within 4-5 days returned to complete soundness. Finally, these horses that tend to have a long toes and under run heels need to be trimmed and re-set every 4-5 weeks. It is quite common that these horses are sound for the first 4 weeks after the farrier visit yet their performance begins to diminish as 5 to 6 weeks pass before they are trimmed and re-set. Although radiographs are not necessary to diagnose this problem, they are helpful for quantifying the extent of imbalance and documenting improvement after shoeing. |
 |
| Figure 4 |














































