Two adult horses presented to PHD Veterinary Services this Fall/winter for very different complaints yet the same disease process. Horse #1 was a 10 year-old gelding that presented for the complaint of rearing under saddle and refusing to go forward. Horse #2 was a 5 year-old mare that presented for the complaint of recurrent low grade colic after eating. A gastroscopy was performed on both horses and both horses were diagnosed with gastric ulcers. In Figure 1, the area of ulceration is within the blue circle and the ulcerated tissue is highlighted by the red arrows. The ulcers in Figure 1 correspond to the horse which was rearing and the ulcers scored a 3 out of 5 with 5 being severe. In Figure 2 and 3, the ulcers appear less severe (score 2/5) and correspond to the horse that was demonstrating abdominal pain after eating. Interestingly, the gastric ulcers in the horse that was rearing under saddle appear worse than the horse with recurring symptoms of colic.
,
,
 |
| Figure 1 |
 |
| Figure 2 |
 |
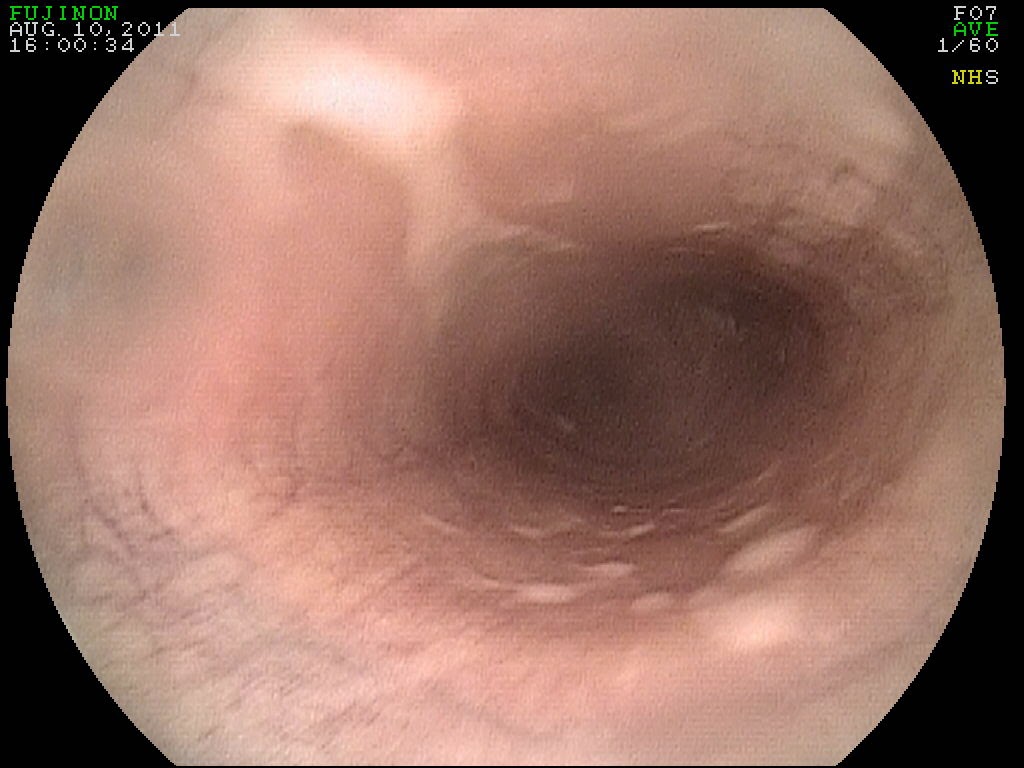
| Figure 3 |
In Figure 4, a "normal stomach" is imaged through gastroscopy. The horse's stomach can be divided into the glandular stomach (darker red tissue) and the non-glandular stomach (lighter tissue). The junction of the two types of tissue (yellow arrows) is called the margo plicata. Most gastric ulcers in horses occur at the margo plicata and in the non-glandular stomach immediately adjacent to the margo plicata.
Listed below are a list of clinical symptoms which can fit with gastric ulcers in horses:
1- Recurring colic
2: Weight loss and failure to thrive
3: Poor performance
4: Sudden change in behavior
5: Unwilling to go forward
6: Rearing under saddle
7: Increased sensitivity to brushing/touching of abdominal and flank area
8: Repeated straining to urinate: parking-out for geldings and tail flagging for mares
The take home message is that gastric ulcers can present in many different ways and should always be considered when evaluating horses for performance/behavior issues.





















.JPG)



















{kind=link}